.webp)
The connection between an in-house dental laboratory and implant success is not simply about convenience or speed. It is about the accuracy of the prosthesis that is attached to the implants — and how that accuracy affects the biological and mechanical outcomes that determine whether the implants succeed for 10–20 years or begin to fail within a few.
Passive Fit: The Critical Prosthetic Requirement for Implant Bridges
An implant-supported bridge must achieve passive fit — meaning that when the bridge is placed on the implant abutments without any screws tightened, it rests in position with zero applied stress. When a bridge does not achieve passive fit, tightening the screws deforms the bridge slightly, applying a constant mechanical stress to the implant-abutment interface and to the implant bodies themselves. This stress does not disappear when the patient is not chewing; it is always present.
The consequences: screw loosening (the most common early complication of implant-supported bridges); marginal bone loss (the stress concentration at the implant neck accelerates crestal bone remodelling); and in severe cases, implant fracture at the neck. Published data: misfit in the range of 100–300 microns creates measurable stress at the implant neck that is clinically significant over years of function. For more on how the in-house lab fabricates these bridges, see our digital lab technical guide.
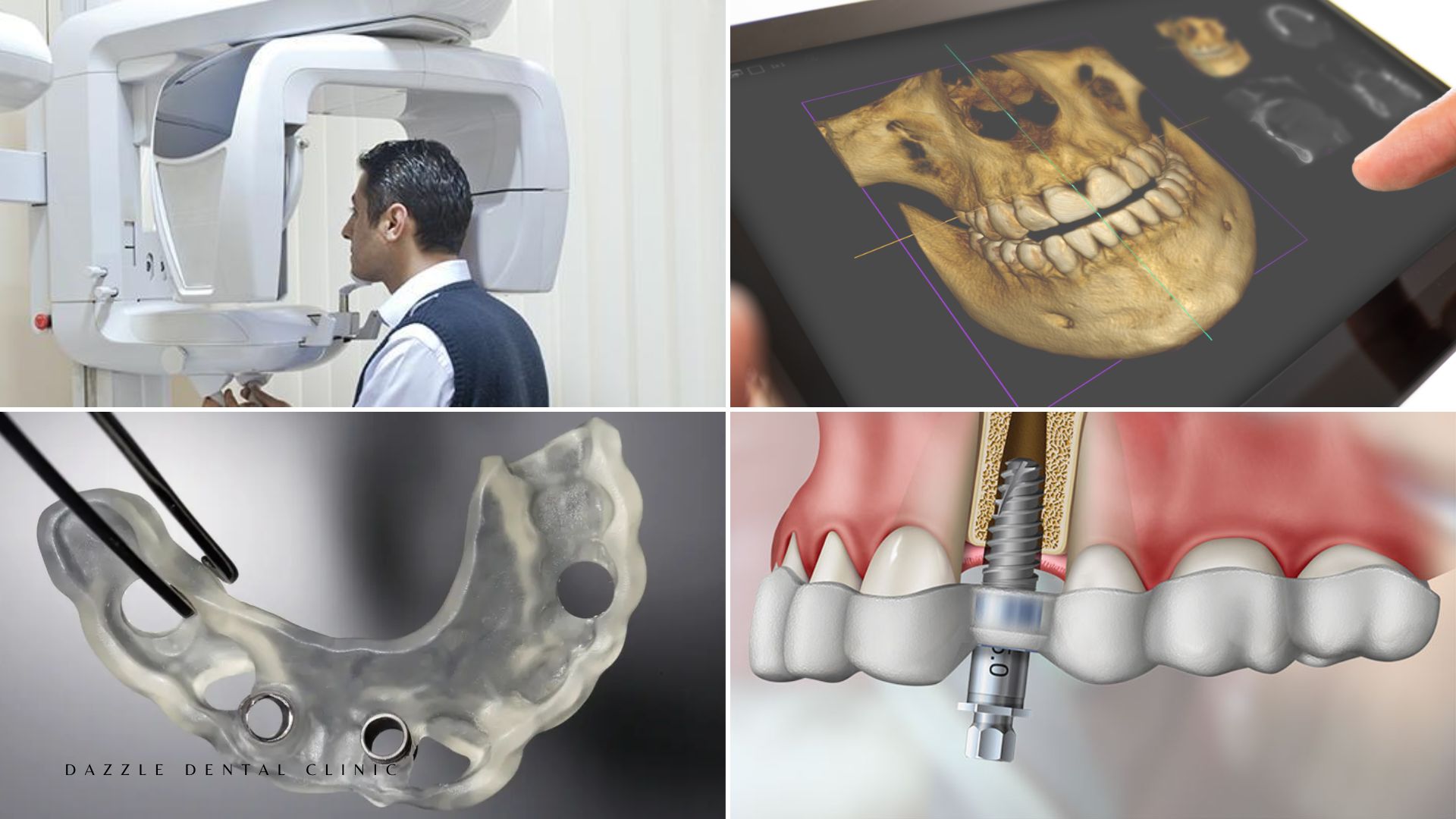
Passive fit in a multi-implant bridge is achieved through accurate digital impression data (intraoral scan), precise design, and milling tolerances measured in microns. The TRIOS intraoral scanner at Dazzle captures scan data with dimensional accuracy that physical impressions in complex implant cases cannot reliably match — particularly over long bridge spans where the cumulative error in a physical impression compounds across the full arch.
Abutment Selection and Emergence Profile Design
The abutment is the component connecting the implant body (in the bone) to the prosthetic crown or bridge above. Its design — height, angle, and emergence profile — determines the shape of the soft tissue around the implant, which in turn determines peri-implant health.
Custom abutments (designed digitally from the intraoral scan and the implant position) allow the emergence profile to be tailored to the patient’s specific gum architecture, supporting the soft tissue in a way that stock abutments — which come in fixed sizes from the implant manufacturer — cannot. Custom CAD/CAM titanium abutments designed and milled in Dazzle’s laboratory have the emergence profile the patient’s tissue requires, not the closest available stock size.
This is particularly significant for anterior single implants in the aesthetic zone, where the emergence profile determines the papilla height and gum margin position — both highly visible and difficult to correct after the fact if the abutment design is suboptimal.
Occlusal Design and Load Distribution
Unlike natural teeth, implants have no periodontal ligament. There is no proprioceptive feedback telling the patient they are biting too hard on a specific implant. Implant-supported prostheses must be designed with calibrated occlusal contacts that distribute bite forces evenly across all implants and avoid damaging concentrations on individual fixture sites.
This occlusal design is done in the CAD software before milling. The prosthodontist reviews the contact pattern digitally before the bridge is fabricated and specifies the occlusal scheme. Intraoperative digital articulation at Dazzle confirms the contact pattern after cementation, allowing immediate adjustment if any single implant is carrying more load than the design intended.
What In-House Lab Control Means for Implant Outcomes
When implant cases are outsourced to external labs, the communication of what is needed — emergence profile, abutment angle, bridge contour, occlusal scheme — passes through written instructions and physical models. At Dazzle, the implantologist and prosthodontist discuss the design directly with the technician, review the digital design on screen before fabrication, and can make adjustments immediately if the design is not correct. This compression of the feedback loop between clinical decision and fabrication execution is what the in-house lab changes for implant outcomes specifically.
FAQs
Q1: How do I know if my implant bridge fits passively?
Passive fit is confirmed clinically by placing the bridge without screws and checking that it seats fully on each abutment simultaneously without rocking or requiring pressure to seat. Periapical radiographs confirm the bridge-abutment gap is closed at each implant. At Dazzle, passive fit is confirmed before final screw tightening on every multi-implant case.
Q2: What is the difference between a stock abutment and a custom abutment?
Stock abutments are manufactured by the implant company in fixed geometries and sizes. Custom abutments are designed individually from the intraoral scan and milled to the exact emergence profile and angle needed for that patient’s implant position and soft tissue anatomy. Custom abutments cost more but produce better soft tissue support and emergence aesthetics, particularly for anterior implants.
Q3: Can occlusal problems after implant bridge placement cause implant failure?
Yes. Persistent heavy occlusal load on a single implant — particularly lateral forces from an off-balance occlusal scheme — can cause crestal bone loss and eventually implant failure. This is most commonly an issue with cantilever extensions or bridges where one implant is taking disproportionate load. Occlusal analysis and adjustment at placement and at 3-month review prevents this.
Q4: How often should implant prosthetics be checked after placement?
Review at 3 months post-placement (osseointegration confirmation), 6 months, and annually thereafter. At each review: screw torque check, peri-implant probing, periapical radiograph to confirm marginal bone levels, occlusal assessment. The annual radiograph is the primary tool for detecting early marginal bone loss before it becomes clinically significant.