.webp)
Full mouth restoration — also called full mouth rehabilitation — is a comprehensive approach to restoring the health, function, and aesthetics of the entire dentition when multiple teeth are damaged, missing, worn, or failing simultaneously. The defining challenge is that the problems are interconnected: you cannot restore the upper teeth without considering how they bite against the lower; you cannot place implants without first managing periodontitis; you cannot fabricate final crowns until the vertical dimension of occlusion is established. Sequential, independent single-specialist treatment does not produce a coordinated outcome. A multi-disciplinary team that plans together does.
Who Needs Full Mouth Restoration
Full mouth restoration is appropriate for patients with: extensive tooth loss requiring multiple implants and a coordinated prosthetic plan; severe generalised tooth wear from bruxism, acid erosion, or attrition where the vertical dimension has been lost; multiple failing teeth from untreated decay, failed restorations, or periodontitis; patients converting from removable dentures to fixed implant-supported prostheses; and patients who have deferred dental care for an extended period and present with problems across multiple quadrants simultaneously.
It is not the appropriate framework for isolated problems. A patient with one failing crown and otherwise healthy teeth does not need full mouth restoration — and presenting it as such is not appropriate care planning.
The Multi-Disciplinary Team Model at Dazzle
At Dazzle Dental Clinic, full mouth restoration cases are assessed and planned by the appropriate specialists together rather than in sequence. The roles:
Prosthodontist: Coordinates the overall restorative plan, establishes the final prosthetic outcome (tooth positions, vertical dimension, occlusal scheme), and fabricates or oversees fabrication of all final restorations. The prosthodontist’s plan determines what every other specialist is working toward.
Periodontist: Assesses and treats gum disease and bone loss before restorative work begins; manages peri-implant soft tissue; performs gum grafting and crown lengthening where the restorative plan requires modified gum architecture.
Endodontist: Assesses teeth with pulpal or periapical pathology and determines whether root canal treatment or extraction is the appropriate decision. This decision directly affects the prosthodontist’s implant placement plan.
Oral surgeon / Implantologist: Performs extractions, bone grafting, and implant placement guided by the prosthodontist’s prosthetic plan — implants are placed in the positions the prosthesis requires, not in the positions that happen to be simplest surgically.
This team works from a shared master plan. When the periodontist treats bone defects, they know what implant positions are planned. When the surgeon places implants, they know the prosthetic emergence angles required. When the prosthodontist fabricates the final restorations, they know what the preceding treatment has achieved.
The Provisional Phase: Why It Cannot Be Skipped
In full mouth restoration cases, a provisional restoration phase is not optional. After the preparatory treatment (periodontal, endodontic, surgical) is complete and before final restorations are fabricated, provisional crowns, bridges, or full-arch prostheses are placed to establish the planned vertical dimension and aesthetic outcome in function.
The patient wears these provisionals for 4–8 weeks while the jaw muscles and joint adapt to the new vertical dimension and the patient evaluates the aesthetic result. Changes to tooth shape, length, or colour that emerge during the provisional phase are incorporated into the final fabrication. This step prevents the most costly outcome in full mouth restoration: a final restorative result that does not function or look right, requiring extensive remake.
Timeline and What Patients Can Expect
Full mouth restoration is not completed in a single appointment or even a few weeks. For cases involving implants, the total treatment span covers the osseointegration period (3–6 months). For non-implant cases, the span is determined by the number and type of procedures required. A realistic minimum for a comprehensive full mouth restoration involving implants: 4–6 months from start to final prosthesis delivery. For international patients, this is structured into 2–3 planned visits.
FAQs
Q1: How is full mouth restoration different from a smile makeover?
A smile makeover focuses primarily on aesthetics — veneers, whitening, gum reshaping — on teeth that are structurally healthy. Full mouth restoration addresses functional and structural problems (missing teeth, bone loss, failed restorations, lost vertical dimension) alongside aesthetics. The planning framework and treatment sequence are different even when the aesthetic outcome looks similar.
Q2: Does full mouth restoration always involve implants?
No. If the patient has no missing teeth and the restoration involves crowns, bridges, or veneers across multiple quadrants, implants are not required. Implants are part of full mouth restoration when missing teeth need to be replaced as part of the comprehensive plan.
Q3: Can full mouth restoration be done in phases for financial reasons?
Yes, with careful planning. The master plan is established upfront, and treatment is phased with interim provisional restorations protecting untreated teeth. Phasing must be planned so that what is treated in phase one is not compromised by postponing phase two — this requires the full plan to be designed before any treatment begins, not decided incrementally.
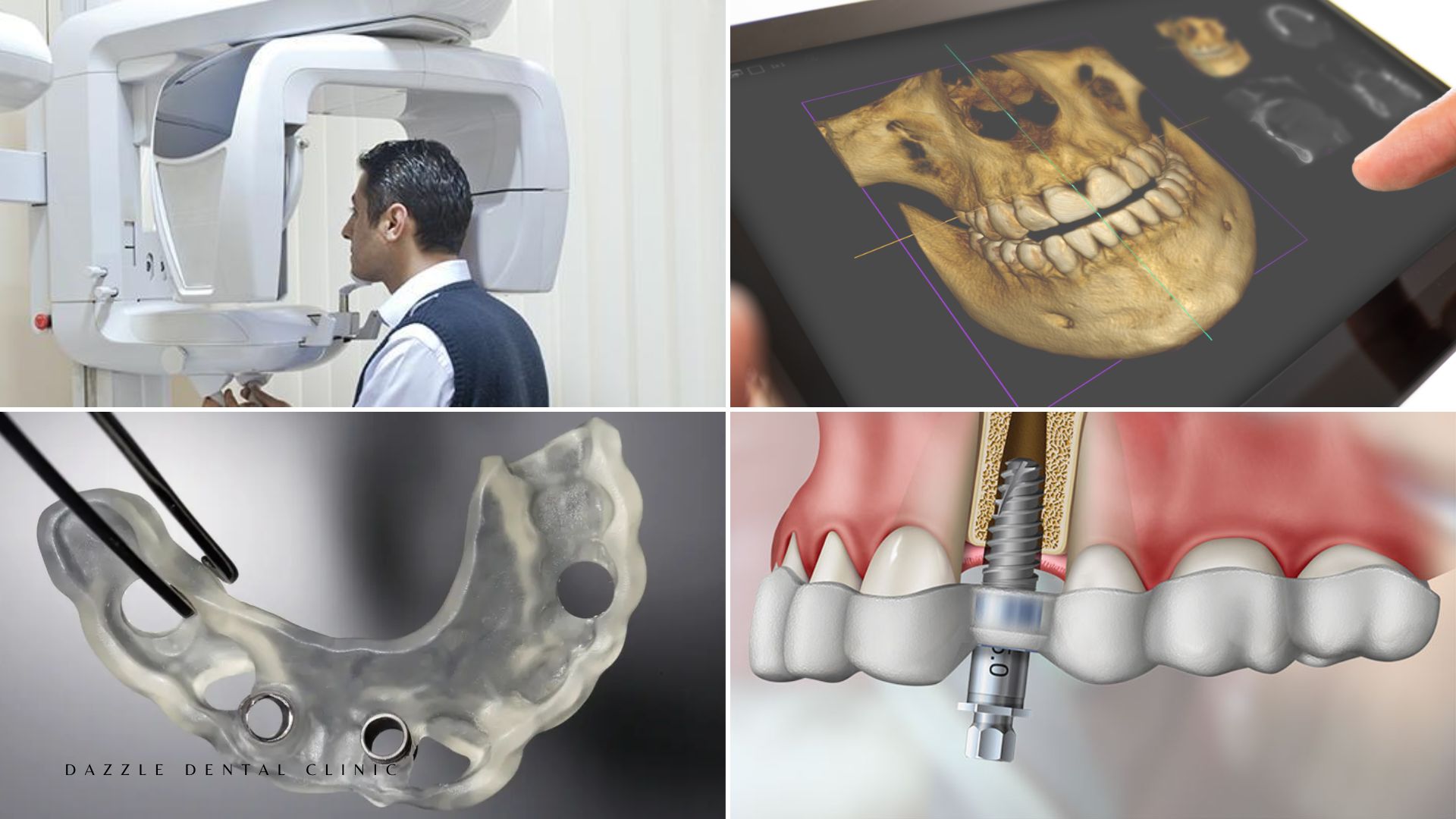
Q4: What happens at the initial full mouth restoration consultation at Dazzle?
Comprehensive assessment: full-mouth clinical examination, full-mouth radiographic series, CBCT where implant planning is anticipated, digital intraoral scan, and photographs. From this dataset, the multi-disciplinary team reviews the case and develops a master treatment plan with a sequenced treatment timeline and full itemised cost. This consultation appointment is typically 60–90 minutes.