.webp)
Bone grafting is probably the most misunderstood part of the All-on-4 journey. Some patients have been told they need it and don’t know what it means. Others have been told they can’t have implants because of their bone, and don’t realise grafting might solve the problem. And many patients who go ahead with All-on-4 don’t need grafting at all — which is one of the technique’s defining advantages.
This article explains what bone grafting actually is, when it’s genuinely necessary for implant success, what types are available, and how it fits into the overall treatment timeline at Dazzle Dental Clinic.
What Bone Grafting Does
Bone grafting is a surgical procedure that adds bone material to an area of the jaw where volume or density is insufficient to support an implant. The graft material acts as a scaffold — it occupies the space and triggers the body’s natural bone-forming cells (osteoblasts) to deposit new bone around and through it. Over time, the graft integrates with the existing jawbone, increasing the volume and density at the implant site.
The goal is not simply to add bulk — it’s to create conditions in which an implant can achieve the primary stability (initial mechanical fixation) necessary for osseointegration to proceed. An implant placed in bone that can’t hold it adequately will fail, regardless of technique.
When Bone Grafting Is and Isn’t Required for All-on-4
One of All-on-4’s defining features is its ability to work around areas of bone loss. The angled posterior implants engage the denser anterior bone and avoid the posterior maxilla where sinus pneumatisation is most pronounced. This design means that many patients who would require bone grafting for conventional implant placement can undergo All-on-4 without it.
That said, grafting is sometimes necessary:
Socket grafting at extraction sites: When failing teeth are extracted in preparation for implants, the sockets may be grafted to preserve ridge width and prevent collapse during healing. This is a smaller, more localised procedure than major jaw grafting.
Ridge augmentation: In cases where the alveolar ridge has resorbed significantly in width or height — leaving a narrow, knife-edge ridge — grafting may be required to create enough bone volume for implant placement, even with angled posterior positioning.
Sinus lift (maxillary sinus augmentation): When the posterior upper jaw has lost significant height and the maxillary sinus has expanded downward, a sinus lift adds bone beneath the sinus membrane to create vertical height for implant placement. This is the most common grafting procedure needed for upper arch implants.
Patients with severe maxillary bone loss who cannot be treated even with grafting may be candidates for zygomatic or pterygoid implants — which bypass the deficient bone entirely.
Types of Bone Graft Material
Autograft (patient’s own bone) remains the biological gold standard. Bone harvested from the chin, ramus, or tibia contains living osteogenic cells that integrate rapidly and predictably. The trade-off is a second surgical site, which adds recovery complexity. Autografts are typically reserved for larger volume deficiencies where other materials are insufficient.
Allograft (donor bone) is processed human bone from a tissue bank, sterilised and demineralised to eliminate biological risk while preserving its structural matrix. It stimulates bone formation without the need for a donor site. Allografts are widely used for socket preservation and moderate augmentations.
Xenograft (bovine-derived bone) — most commonly Geistlich Bio-Oss® — is a highly purified bovine bone mineral used extensively in implant dentistry. Its slow resorption rate makes it useful as a space maintainer in sinus lifts and ridge augmentations, providing a stable scaffold as new bone forms around it. It has an excellent published safety and efficacy record.
Synthetic grafts (hydroxyapatite, β-TCP) are biocompatible calcium phosphate materials that resorb over time as bone replaces them. They are suitable for contained defects and smaller augmentations.
PRF: How the Body’s Own Growth Factors Accelerate Healing
Platelet-Rich Fibrin (PRF) is derived from the patient’s own blood by centrifugation. The resulting membrane or liquid concentrate is rich in growth factors — PDGF, TGF-β, VEGF — that accelerate soft tissue healing, enhance angiogenesis (new blood vessel formation), and improve bone regeneration at the graft site.
At Dazzle Dental Clinic, PRF is routinely incorporated into bone grafting procedures and implant surgeries. It’s mixed with graft material or applied as a membrane over the surgical site. The benefit is measurable: faster initial healing, reduced post-operative discomfort, and improved graft incorporation. Because it’s derived from the patient’s own blood, there is no immunological reaction or rejection risk.
How Bone Grafting Affects Your Treatment Timeline
This is the practical question most patients want answered. The timeline impact depends on what type of grafting is required:
Socket preservation grafts at extraction sites require 3–4 months of healing before implants can be placed in those sites. In some cases, implants can be placed simultaneously with extraction and socket grafting.
Sinus lifts require 4–6 months of healing before implants can be placed in the augmented area. This extends the overall treatment timeline but doesn’t change the endpoint.
Major ridge augmentation may require 6–9 months before implant placement is appropriate.
We explain this timeline clearly at consultation — not as a reason to delay, but so patients can plan accurately. Provisional prostheses are provided throughout, so patients are never without teeth during the waiting period.
Getting the Right Assessment
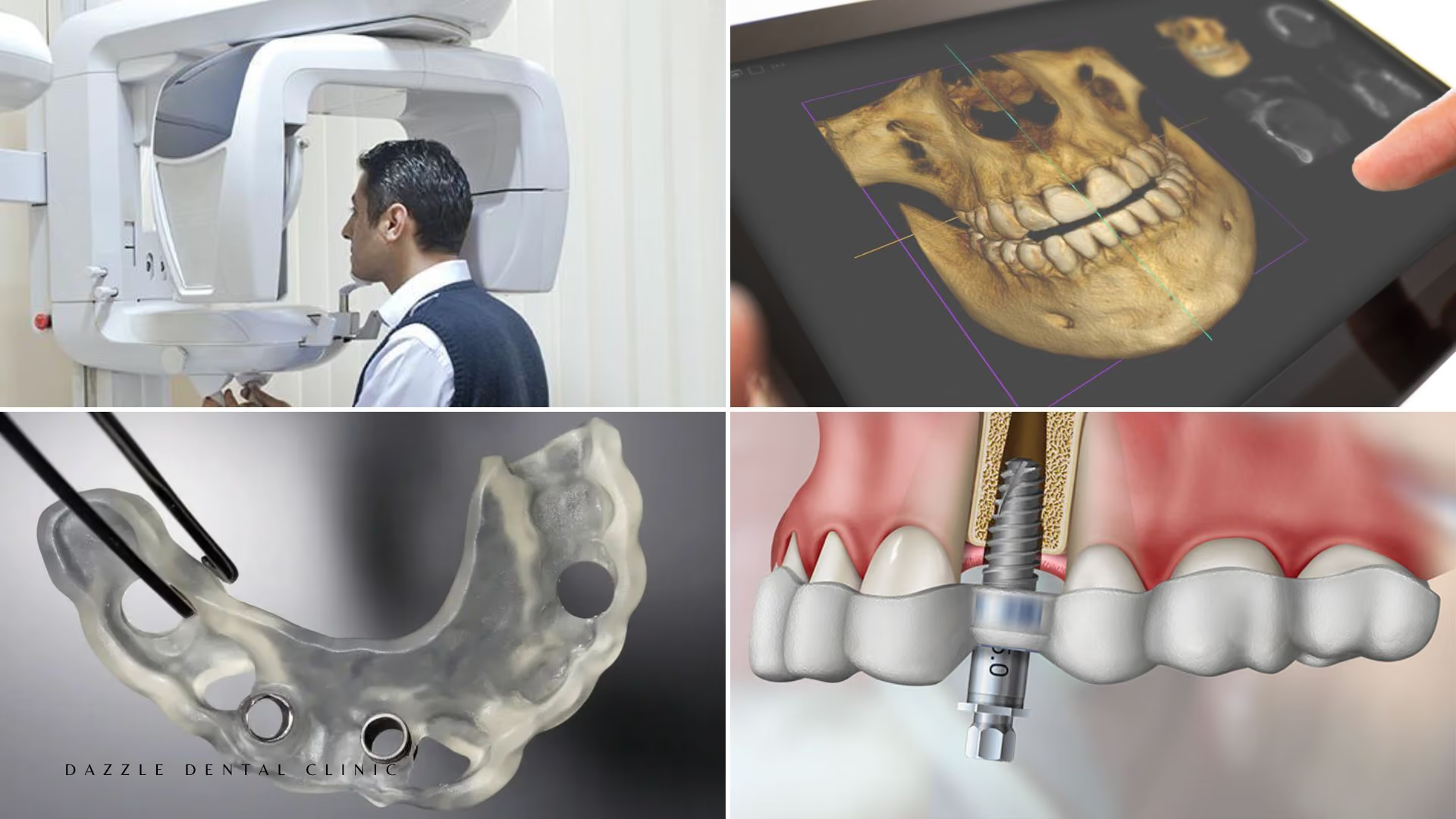
Whether you need bone grafting cannot be determined without a CBCT 3D scan. Panoramic X-rays show bone height in 2D but cannot accurately convey width or density. Patients told they “need bone grafting” based on a 2D image alone should request 3D imaging before accepting that assessment as final. And patients told grafting is impossible should consider whether zygomatic or pterygoid implant alternatives have been properly explored.
Book a consultation at Dazzle Dental Clinic — in person or by submitting your existing CBCT remotely — and we’ll give you a specific, clear answer about what your case actually requires.
FAQs
Q1: Does All-on-4 always require bone grafting?
No. The All-on-4 design specifically reduces or eliminates the need for bone grafting in many patients. The angled posterior implants work around areas of bone deficiency. Whether any grafting is needed depends on your specific bone volume and the proposed implant positions, assessed on CBCT imaging.
Q2: Is bone grafting painful?
Grafting is performed under local anaesthesia. The procedure itself is not painful. Post-operative discomfort varies depending on the size and location of the graft — socket grafts are typically mild; larger augmentations may involve more swelling and discomfort for several days, managed well with prescribed medication.
Q3: Does bone grafting change how long the whole treatment takes?
Yes, in most cases. Depending on the type of graft, you may need 3–6 months of healing before implants can be placed in the grafted site. The overall treatment is longer, but the endpoint — a fixed, full-arch implant restoration — is the same. We provide provisional teeth throughout.
Q4: What is PRF and do I need it?
PRF (Platelet-Rich Fibrin) is a healing concentrate made from your own blood that’s added to bone graft procedures to accelerate healing and improve graft success. It’s not a requirement, but it’s something we routinely recommend and use at Dazzle because the evidence for its benefit is well-established and the addition is low-risk.