.webp)
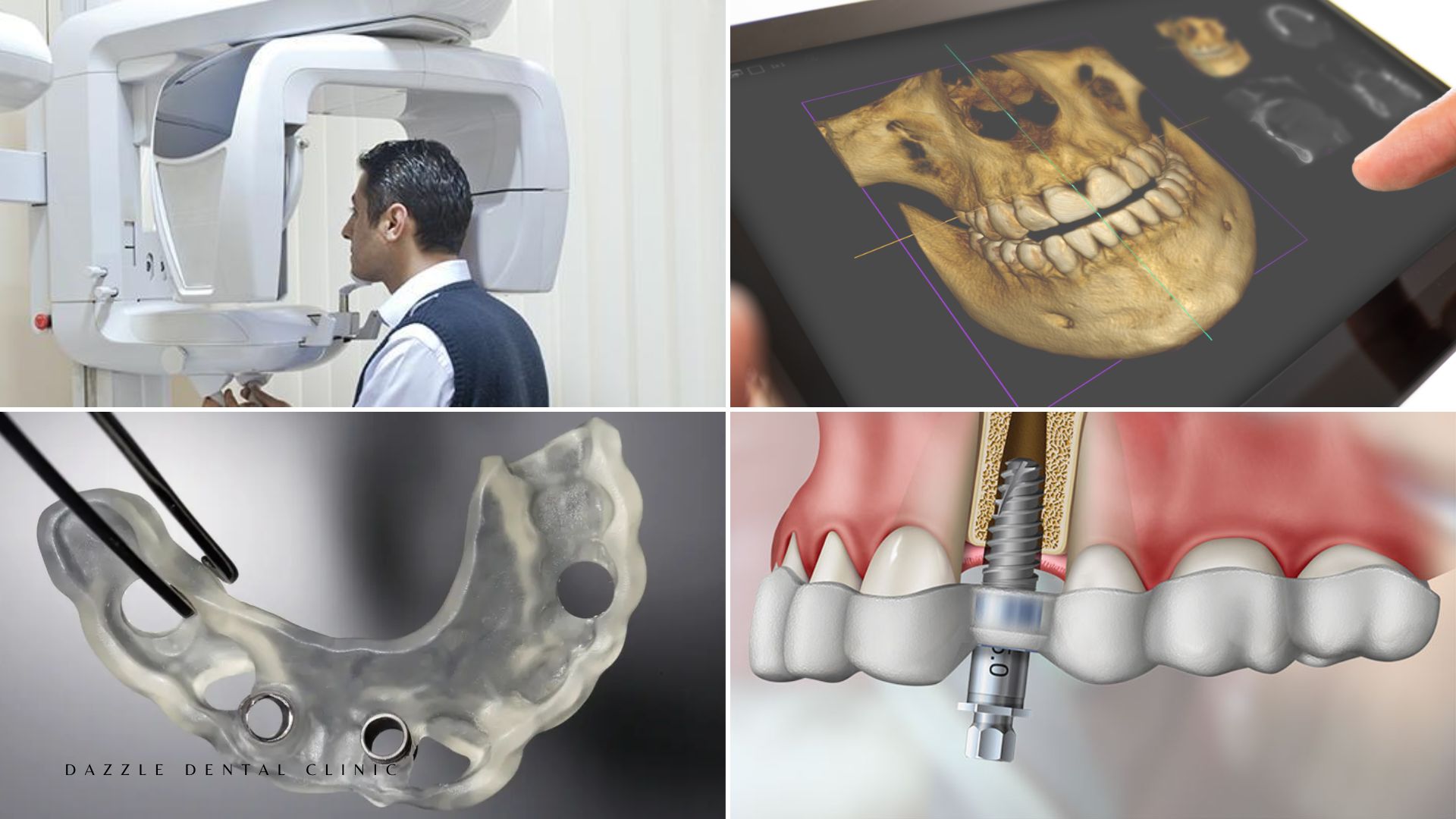
Same-day implant treatment — leaving the clinic with fixed provisional teeth on the day of surgery — is well established for conventional All-on-4 cases in good bone. What is less widely understood is that the same outcome is achievable for patients with severe bone loss through zygomatic and pterygoid implant approaches, and that the mechanism enabling this is fundamentally different from conventional immediate loading.
Why Bone Loss Normally Prevents Same-Day Conventional Implants
Immediate loading in conventional All-on-4 requires primary stability — measured as insertion torque ≥35 Ncm and ISQ ≥60. In severely resorbed alveolar bone (Misch Type III–IV), the trabecular lattice offers insufficient mechanical resistance. Insertion torque falls below threshold, micromotion under the provisional bridge occurs, and the bone-implant interface forms fibrous tissue instead of bone. The implant fails. This is why patients with severe bone loss are often told they need bone grafting — requiring 12–18 months before fixed teeth.
Why Zygomatic Implants Change the Same-Day Calculation
Zygomatic implants anchor in the zygomatic bone (cheekbone) — which is predominantly cortical, dense, and entirely unaffected by alveolar resorption. Insertion torque in the zygomatic body consistently exceeds 35 Ncm regardless of the patient’s alveolar bone condition. The primary stability that enables immediate loading comes from the cortical zygomatic bone, not from the deficient alveolar ridge. A patient with virtually no posterior alveolar bone can have zygomatic implants placed with measured primary stability that exceeds immediate loading thresholds, and a provisional bridge fitted on the same day.
Pterygoid implants work on the same principle: the pterygoid plates are dense cortical bone that provide reliable high-torque anchorage in the posterior maxilla, enabling same-day loading of the posterior arch positions without sinus involvement.
What the Treatment Day Looks Like
Surgery for a full-arch zygomatic case takes 3–5 hours under local anaesthesia and IV sedation. The sequence: any remaining teeth are extracted; zygomatic implants (and any conventional anterior implants) are placed; insertion torque and ISQ are measured for each implant; where all implants meet immediate loading criteria, the provisional bridge is screwed into place. The patient leaves with a fixed provisional bridge that functions for eating soft foods from day 1.
The provisional bridge placed at surgery is not the final restoration. The final bridge — in zirconia or acrylic-on-titanium frame — is delivered at 3–6 months at the second visit.
International Patient Logistics for Single-Day Cases
For patients travelling to Dazzle from the UK, Australia, the UAE, or East Africa, the single-day surgical approach concentrates the surgical event into one visit: consultation on day 1; surgery on day 2 or 3; recovery days 3–5; departure from day 5–7 with provisional bridge in place. Final bridge delivery at visit 2, approximately 3–5 months later, takes 2–3 days in Mumbai.
FAQs
Q1: Is same-day treatment guaranteed, or could it not happen on the day?
Not guaranteed. Primary stability is measured intraoperatively — if any implant falls below the immediate loading threshold, that implant is placed on a healing protocol rather than incorporated into the immediate loading bridge. This is communicated pre-surgically as a possibility.
Q2: How soon after surgery can I eat?
Soft, cool foods from later the same day: yoghurt, soup, soft scrambled eggs, smoothies. Nothing hot for 24 hours. Soft diet maintained for 6–8 weeks.
Q3: Can the provisional bridge break during the healing period?
Composite provisional bridges can fracture at thin sections, particularly if hard food is eaten against the surgeon’s advice. Patients are advised not to bite hard foods with the provisional and to follow the food guide provided.
Q4: Why is the second visit necessary — can the final bridge not be placed at surgery?
The final bridge requires osseointegration to be confirmed before it is fitted. The provisional bridge is the insurance: if an implant fails during healing, it is managed before the final bridge is fabricated, saving the cost and time of remaking a high-quality final restoration.