.webp)
Temporomandibular disorders (TMD) are a group of conditions affecting the temporomandibular joint (TMJ), the masticatory muscles, or both. The TMJ connects the lower jaw (mandible) to the temporal bone of the skull on each side, allowing the jaw to open, close, and move laterally for chewing and speaking. It is one of the most complex joints in the body. At Dazzle Dental Clinic, our TMJ/TMD specialist treatment and dental check-up assess patients for signs of dysfunction early.
What Causes TMD?
TMD is rarely caused by a single factor. The most common contributors are parafunctional habits (bruxism — grinding; clenching); malocclusion (misaligned bite); trauma to the jaw or joint; disc displacement within the joint; arthritis (osteoarthritis or rheumatoid arthritis affecting the TMJ); and psychological stress, which increases muscle tension and parafunctional activity. In many patients, multiple factors interact. This is why TMD management requires a comprehensive assessment rather than a single-symptom approach.
Symptoms of TMD
Joint sounds: clicking, popping, or crepitus (grating) during jaw movement — particularly on opening or closing. Limited mouth opening: reduced range of jaw motion, often accompanied by pain at the end range. Jaw pain or facial pain: particularly at the joint itself (in front of the ear), the temples, or along the masseter muscle (jaw muscle). Headaches: particularly morning headaches on waking, which often indicate nocturnal bruxism. Ear symptoms: earache, tinnitus, or a sense of ear fullness without ear pathology. Tooth wear: uneven, flat incisal edges or posterior cusps, often associated with bruxism. Neck and shoulder pain: referred from chronically tense masticatory muscles.
Diagnosis
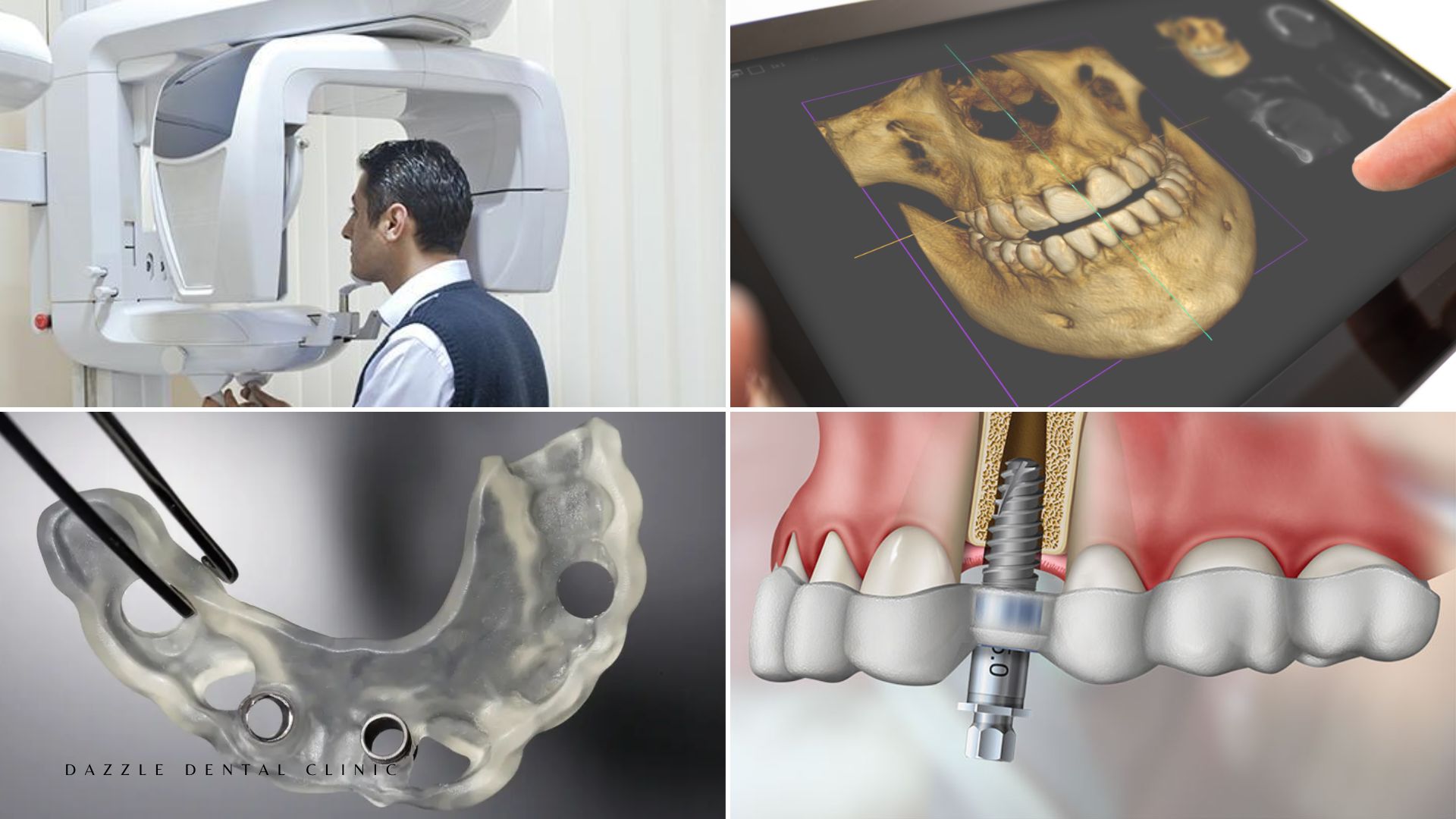
Accurate TMD diagnosis at Dazzle includes: a detailed clinical history; examination of range of jaw motion, joint sounds, and muscle tenderness; occlusal assessment; and imaging where indicated. For detailed occlusal adjustment assessment, see our occlusal adjustment guide. For the connection between occlusal load and implant health, see our occlusal load management guide. CBCT is used where disc displacement, bone changes, or joint anatomy is complex. CBCT of the TMJ provides detailed information on condylar morphology, joint space, and bone changes that is not available from standard X-ray.
Treatment Approaches
Conservative management: First-line for most TMD. Includes: jaw rest (soft diet, avoiding wide opening); NSAIDs for acute pain; heat or cold application to masticatory muscles; physiotherapy for jaw muscle rehabilitation; and patient education on parafunctional habit awareness.
Occlusal splint (nightguard): The most evidence-backed intervention for bruxism-related TMD. A custom hard acrylic splint worn at night redistributes bite forces, reduces muscle activity, and prevents further tooth wear. The splint does not treat the cause of bruxism but effectively manages its mechanical consequences.
Occlusal adjustment: Where specific occlusal interference points are contributing to joint loading, selective occlusal equilibration — minor adjustment of specific tooth contacts — can reduce mechanical stress on the TMJ. This is not a first-line intervention and is used only where specific contacts are clearly implicated.
Botulinum toxin (Botox) for masseter hypertrophy: In patients with masseter muscle hypertrophy from chronic clenching, Botox injection into the masseter reduces muscle bulk and force generation. This is a specialist procedure with a 3–6 month duration of effect per treatment cycle.
FAQs
Q1: How is TMD different from a toothache?
A toothache is localised to a specific tooth and typically associated with tooth pathology (decay, fracture, abscess). TMD pain is typically in the joint or masticatory muscles, reproduced by jaw movement or palpation of the joint and muscle, and not reproduced by percussion of individual teeth.
Q2: Can TMD be permanently cured?
Most TMD is manageable rather than curable in the traditional sense. Many patients achieve long-term symptom control with conservative management and splint therapy. Cases with structural joint damage (disc perforation, condylar resorption) may require more involved intervention.
Q3: Is surgery ever needed for TMD?
Surgery is a last resort for TMD, used only when conservative management has failed and there is specific structural pathology (disc displacement causing irreducible locking, degenerative joint disease with significant functional limitation). The vast majority of TMD patients do not require surgery.
Q4: Does TMD go away on its own?
Many acute TMD episodes resolve within weeks with conservative self-care. Chronic TMD that has persisted for more than 3 months is less likely to self-resolve and benefits from structured management.