.webp)
All-on-6 implants in the upper jaw frequently encounter the same anatomical challenge: the maxillary sinuses limit the bone height available for posterior implant placement. When the sinus floor sits close to the alveolar ridge crest — as it does in many patients who have been edentulous for years — conventional implants placed in the posterior upper jaw would penetrate the sinus cavity. The sinus lift procedure creates the bone height needed to place implants safely. PRF (Platelet-Rich Fibrin) significantly improves how quickly that bone forms and integrates.
What a Sinus Lift Actually Involves
The maxillary sinus is an air-filled cavity in the upper jaw flanked by the cheekbone and the nasal cavity. It is lined by the Schneiderian membrane — a thin, delicate mucous membrane. When the posterior alveolar bone is deficient (as it becomes after tooth loss and sinus expansion), there is insufficient height between the sinus floor and the alveolar crest to place implants of appropriate length.
A lateral window sinus lift (the most common approach) involves creating a small opening in the outer wall of the sinus, gently elevating the Schneiderian membrane away from the sinus floor, and packing the created space with bone graft material. Over the following 6–8 months, this graft integrates with the native bone — creating a new, elevated sinus floor and the bone height required for implant placement.
The critical technical challenge is elevating the Schneiderian membrane without perforating it. Perforation of the membrane during sinus lifting requires immediate repair and can compromise the procedure. At Dazzle, piezoelectric instruments are used for the lateral window creation (their selective cutting action protects the membrane) and the elevation is performed with blunt hand instruments under direct vision.
A minimally invasive alternative — the crestal approach (osteotome technique or balloon sinus lift) — is used when less bone augmentation is required (typically where there is 5–8mm of residual bone). The sinus floor is elevated through the osteotomy rather than a lateral window. This approach has a narrower indication range but offers faster healing when applicable.
Why PRF Changes the Sinus Lift Outcome
The fundamental challenge in a sinus lift is not the surgery itself but the biology: bone graft material (typically bovine xenograft, Bio-Oss) is osteoconductive — it provides a scaffold for bone to grow through, but it does not directly stimulate bone formation. The rate and quality of new bone formation in the grafted sinus depends on the angiogenic and osteogenic signals available in the healing site.
PRF addresses this directly. The growth factors concentrated in the PRF membrane — PDGF, TGF-β, VEGF — drive angiogenesis within the graft mass (new blood vessels bringing oxygen and nutrition to regenerating tissue) and stimulate osteoblast proliferation at the graft-native bone interface. The fibrin matrix also binds graft particles in place, preventing their migration during the early healing phase when particle displacement is a risk.
The clinical evidence: published comparative studies consistently show that sinus lifts using xenograft + PRF produce denser, higher-quality bone at 6 months compared to xenograft alone. Several studies show that the healing period before implant placement can be reduced by 6–8 weeks when PRF is combined with the graft. At Dazzle, Bio-Oss xenograft + L-PRF membrane is the standard sinus lift protocol. Implant placement in the augmented sinus is typically planned at 6 months — sometimes 5 months in cases with excellent PRF-enhanced healing.
When Sinus Lifting Is Necessary vs. Avoidable
Not all upper jaw All-on-6 cases require a sinus lift. The All-on-4 and All-on-6 protocols are specifically designed to avoid sinus lifting in many patients by angling the posterior implants anteriorly — placing their apices in the denser bone anterior to the sinus. When adequate anterior bone is present, angled posterior implants make sinus lifting unnecessary.
Sinus lifting becomes necessary when: the residual bone height in the posterior sites is insufficient even for angled implants; when the All-on-6 design requires more posterior support than angled anterior implants can provide; or when six-implant distribution for the prosthesis design requires posterior placement.
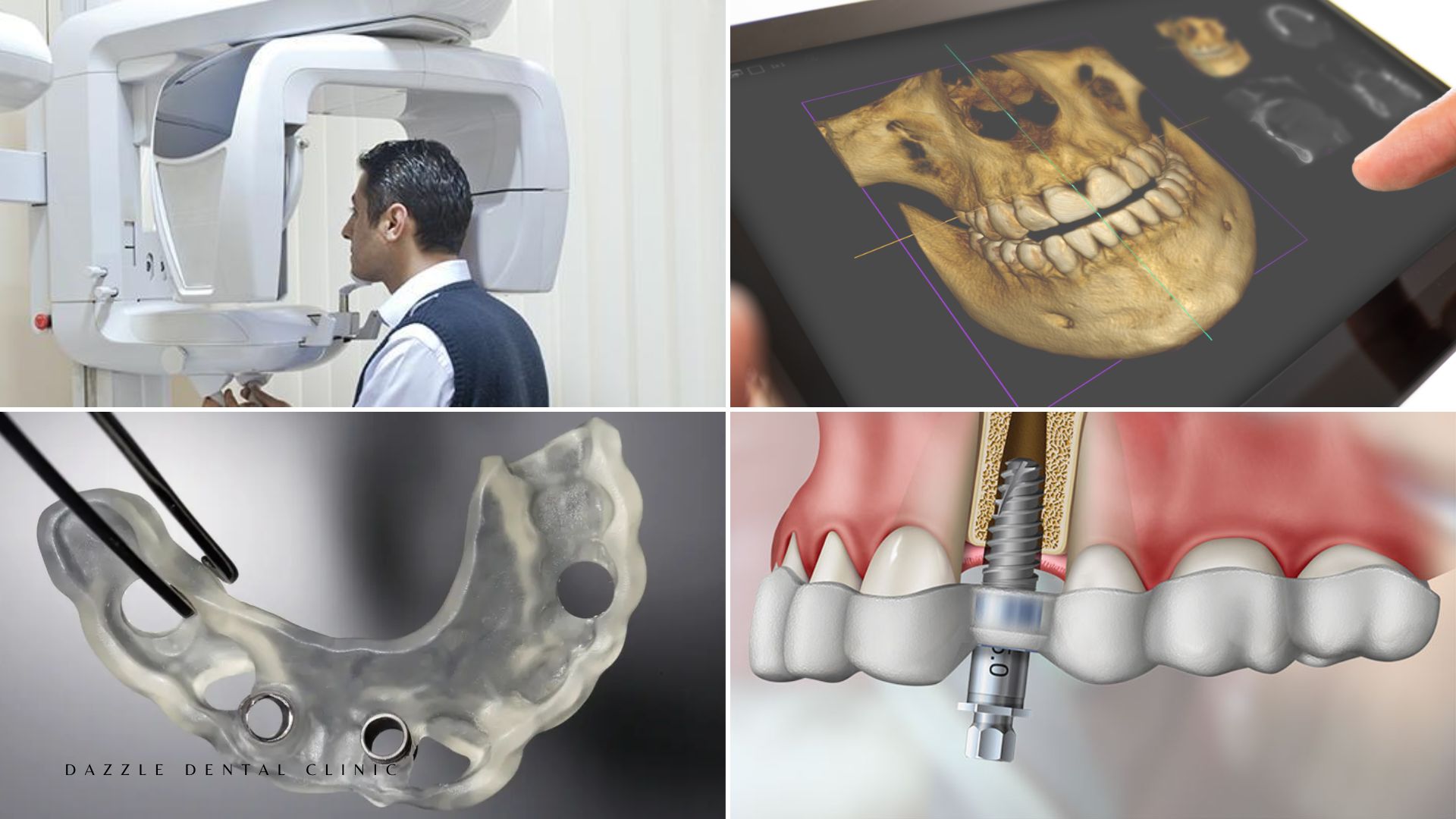
At Dazzle, the surgical plan for every All-on-6 case is based on CBCT assessment. Whether a sinus lift is indicated, optional, or unnecessary is determined by measuring the available bone at each proposed implant site before surgery, not assumed.
All-on-6 vs All-on-4: The Implant Number Decision
All-on-6 uses six implants per arch; All-on-4 uses four. The decision between them is clinical, based on bone distribution, prosthesis design requirements, and the AP spread achievable with the available bone. Six implants provide greater load distribution per implant and more redundancy (if one implant fails, the arch is supported by five rather than three), which is why All-on-6 is sometimes preferred in specific clinical configurations. It is not automatically superior to All-on-4 — in appropriate cases, four well-placed implants perform equivalently.
FAQs
Q1: How long does it take to get teeth after a sinus lift?
If the sinus lift is staged (done before implants, then implants placed at 6 months, then provisional bridge at surgery), the total timeline from sinus lift to fixed teeth is 6–8 months. Some cases allow simultaneous sinus lift and implant placement (when 4–5mm of residual bone provides enough primary stability), which reduces the timeline to 4–6 months to provisional bridge.
Q2: Is sinus lift surgery painful?
Performed under local anaesthesia and IV sedation, the procedure is not painful during surgery. Post-operative swelling of the cheek on the operated side is the primary recovery experience, peaking at 48–72 hours and resolving over 7–10 days. NSAIDs and antibiotics manage discomfort and infection risk during healing. Most patients describe the recovery as more significant than a routine extraction but manageable.
Q3: Can a sinus lift be avoided with zygomatic implants?
Yes. Zygomatic implants anchor in the zygomatic bone and bypass the sinus entirely, making sinus augmentation unnecessary. They are the primary alternative for patients with severe posterior maxillary bone loss where a sinus lift would be the only option for conventional implant placement. The choice between sinus lift and zygomatic implants depends on anatomy, patient preference regarding surgical extent, and timeline. We discuss both options at consultation for appropriate cases.
Q4: Can PRF be used alone without bone graft in a sinus lift?
In small sinus lifts (elevation height of 2–4mm), PRF alone — without additional xenograft — has published evidence for creating adequate bone volume. For larger elevations (5mm+), the combination of xenograft scaffold + PRF is the standard protocol. PRF alone does not provide the physical volume support that graft material offers when larger bone dimensions are required.